
CASE STUDY
Emerging Zoonoses

A 28-year-old man presents to the Emergency Room (ER) in Kerala, India with confusion, fever, and vomiting. His relatives, some of whom catch wild animals and collect fruit, are also in the ER and have similar symptoms.
This case will guide you through a clinical encounter to understand the patient's health challenges – and how to respond.
LEARNING OBJECTIVES
Understand how ecological changes and human-animal interactions contribute to emerging zoonoses
Apply knowledge of the local human-animal interface to identify and prevent emerging zoonotic diseases (diseases transmitted between animals and humans)
CLINICAL COMPETENCIES
Integrate history of animal contacts and environmental exposures in the development of a differential diagnosis that includes zoonoses
Select appropriate diagnostic testing for emerging zoonotic diseases
Understand the origins of zoonotic outbreaks including modes of transmission and sources of spillover
Identify community health interventions that can limit zoonotic disease spread
A Continuing Medical Education activity presented by the Stanford Center for Innovation in Global Health and the University of Washington. View CE information and claim credit HERE.
Accreditation
In support of improving patient care, Stanford Medicine is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
Credit Designation
American Medical Association (AMA)
Stanford Medicine designates this Enduring Material for a maximum of 1.5 AMA PRA Category 1 Credits™.
Physicians should claim only the credit commensurate with the extent of their participation in the activity.
American Nurses Credentialing Center (ANCC)
Stanford Medicine designates this Enduring Material for a maximum of 1.5 ANCC contact hours.
American Academy of Physician Associates (AAPA)
Stanford Medicine has been authorized by the American Academy of PAs (AAPA) to award AAPA Category 1 CME credit for activities planned in accordance with AAPA CME Criteria.
This enduring activity is designated for 1.5 AAPA Category 1 CME credits. Approval is valid until December 14th, 2026. PAs should only claim credit commensurate with the extent of their participation.

Clinical Approach
Consider the following questions as you work through this case:
What animal and environmental exposures has your patient encountered?
Clinical suspicion based on a detailed history of exposures is necessary to detect emerging and endemic zoonoses.
Geography, recreational and professional activities, immune status, and seasonality can give you clues about which pathogen is involved.
How can clinicians detect sentinel cases of zoonotic diseases?
An animal contact history is essential (considering both wild and domesticated animals – and both direct and indirect contact).
Host factor risks for zoonotic disease: “YOPI”: Young (infants/children), Old (elderly), Pregnant, Immunocompromised.
Understanding zoonotic syndromes and diagnostic testing methods can help clinicians detect index cases of emerging zoonoses.
Collaborating with veterinarians, including wildlife veterinarians, can help identify epizootic events and risks from animals in the community.
What community-level interventions can one start to prevent the spread of zoonoses?
Understanding the drivers of spillover and transmission can help you to teach your patients precautionary measures to take when dealing with domesticated animals and wildlife to avoid transfer of disease.

History
Taking a clinical history of your patient yields the following information:
Chief complaint
History of present illness
Past medical & surgical history
Medications
Allergies
Family history
Social & enviromental history ("Social-E")
Review of systems
Discussion
What would you ask next?
What are sources of information about infection risk in the region?
What would be key things to look for on physical examination, and which lab tests would you order?

For someone with fever and altered mental status in South Asia, consider infectious causes of meningitis and/or encephalitis. HIV, tuberculosis, malaria, dengue, Japanese encephalitis, and typhoid fever are widespread in this region. There may also be regional outbreaks of other relevant pathogens. Sources of information about local infection risk and current outbreaks include the CDC travel website, GIDEON, and Healthmap.
Screening questions about animal contact in the patient’s history can lead to more detailed questions. In this case there are suggestions of high-risk animal contacts in the village and patient’s family.
Key Points
CONsider the following as you continue evaluating your patient:
Key History Follow-Up Questions
Asking your patient the following questions gives you this information:
Do you (or family members) have direct or indirect contact with animals at home or at work?
Have you had any contact with sick animals? Has anyone around you been sick?
What kind of housing do you live in? Do you have access to soap and water in the home?
What do you eat / drink? Do you eat / drink unpasteurized dairy? How do you prepare fruits and vegetables?
Have you noticed any insects – or animal or insect bites?
Are you aware of any recent weather or environmental changes?

Physical Exam
When you examine your patient, you learn the following:
General
Head Eyes Ears Nose Throat (HEENT)
Neck
Chest & lungs
Cardiovascular
Abdominal
Musculoskeletal
Extremities
Skin
Neurologic
Discussion
What are some key findings from the history and physical?

Examples of Physical Exam Findings for Zoonotic Disease
Many zoonotic and vector-borne diseases have non-specific presentations. consider the key points below as you develop your diagnosis.
Note: Zoonotic diseases result from infections that are spread between people and animals. Vector-borne diseases result from infections transmitted to humans and other animals by vectors including mosquitoes, ticks, and fleas.
Examples of findings include:
Altered mental status: consider encephalitis (brain inflammation – altered mental status), meningitis (inflammation of meninges – neck stiffness)
Lymphadenopathy: consider plague, bartonella, other
Skin rash: consider some arbovirus infections (dengue), rickettsia, typhoid, jaundice, leptospirosis, others
Skin ulcer or eschar at site of vector bite: consider rickettsia
Eye conjunctival infection: consider leptospirosis, jaundice, others
Pulmonary (pneumonia, shortness of breath): consider plague, hantavirus pulmonary syndrome, influenza
Cardiac arrhythmias: consider Lyme
Joint pain or swelling: consider dengue, brucella, Lyme
Discussion
What labs would you want to order?

Diagnostics
Information that will be helpful in diagnosing your patient:
In this case, complete blood count (CBC), arterial blood gases test (ABG), liver function tests (LFTs), and basic metabolic panel (BMP) all came back normal. Cerebrospinal fluid (CSF) is clear with no cells, normal protein and glucose. A non-contrast head CT showed diffuse cerebral edema. The chest X-ray showed bilateral infiltrates.

Key Points for Lab Diagnostics
Additional considerations to take into account:
Indications from preliminary results:
Complete Blood Count (CBC): aside from total white blood cell (WBC), look for eosinophilia, lymphocytopenia, and thrombocytopenia (some examples)
Eosinophilia: parasitic infection, some fungal infections, tuberculosis
Lymphocytopenia: viral infection (e.g., HIV, dengue), Typhoid, COVID-19
Thrombocytopenia: malaria, dengue, HIV, typhoid, rickettsia, sepsis / DIC
Complete Metabolic Panel: pay attention to elevated liver function tests, which may indicate viral hepatitis
Additional testing:
If you suspect brucellosis: take two sets of blood cultures before offering any antibiotics, alert the microbiology lab if you suspect brucellosis
If you suspect malaria: 3 sets of thick and thin blood smears (separated by 12-24 hours) AND rapid diagnostic testing (RDT)
If you suspect leptospirosis: look for proteinuria and hematuria using a urine analysis (UA) and send leptospirosis serology and PCR (urine and serum)
Offer HIV testing to patients
In a case of severe unexplained infection, you should also consider performing PCR, multiplex PCR, or next generation sequencing (NGS).
Nested RT-PCR has been developed to improve sensitivity but can be subject to contamination.
Next generation sequencing is becoming more available for molecular epidemiology.
Serological tests, such as ELISA antibody testing, can be considered but often lack specificity due to cross-reactivity, and there can be a lag before antibodies are detectable. Therefore, serology may not be as useful during the acute phase.
Saving both early and convalescent phase samples can be helpful for future testing.
Virus isolation may only be available in certain reference labs (i.e., CDC). It is considered the gold standard but is quickly giving way to PCR.
*Note: not all of these diseases are zoonotic; important for differential diagnosis.
Framework for emerging zoonotic virus diagnostics:


Differential Diagnosis
For altered mental status, fever, and respiratory distress, here are some etiologies you should consider:
Bacterial infection: bacterial meningitis, including meningococcemia, leptospirosis, melioidosis, TB
Viral infection: HIV, rabies, viral hemorrhagic fevers (VHFs), Nipah virus, herpes viruses, coronaviruses
Parasitic infection: Plasmodium falciparum malaria
Opportunistic pathogens if immunocompromised (e.g., HIV/AIDS, etc.)
Other causes of sepsis: recall that altered mental status (AMS) doesn’t always mean the site of infection is in the nervous system

The patient was intubated and admitted to the ICU, started on acyclovir and ceftriaxone. He rapidly deteriorates and dies within 24 hours while diagnostic tests are pending. Endotracheal tube secretions later come back positive for Nipah virus via RT-PCR.
Hospital Course & Diagnosis
what happens next:


Discussion
How do we treat Nipah virus?
There is no licensed treatment of Nipah virus specifically, so management will consist of supportive care. Monoclonal antibodies are undergoing clinical trials. Important parts of management are isolation of the patient and infection control measures.
Management & Treatment
considerations for patient management:

Reducing host vulnerability / susceptibility (host factors):
Recognize host risk factors: Young, Old, Pregnant, Immunocompromised
Optimize health status and immune status
Reducing exposures / improving environments (environmental factors):
Infection control practices: isolating sick family members, modifying burial practices (to reduce contact with the body- if indicated), hand washing, mask use
Preventing food contamination (e.g., using bamboo skirts to prevent bat access to date palm sap, cooking at higher temperature)
Limiting contact between wildlife and humans and domesticated animals (dogs, cats, livestock, poultry)
Not consuming date sap
Have veterinarians report potentially sick animals
Prevention
How can nipah virus infection be prevented?

Beyond the Clinic
Your patient's story is part of a bigger picture:
Nipah virus is a paramyxovirus and single-stranded RNA virus. Pteropid fruit bats (flying foxes) are the reservoir host, and humans have been infected via consumption of fruit/date palm sap contaminated by bat urine/saliva and by butchering/farming infected pigs. Human-to-human transmission is primarily via contact with bodily fluids, also possible aerosol transmission; therefore, close contacts, healthcare workers, and lab workers are at high-risk of exposure. Nipah virus leads to a rapidly progressive severe illness with CNS and respiratory symptoms.
Zoonotic disease spillover occurs when a pathogen is first transmitted between two species. The primary case is the first person originally infected (in this case, likely the patient’s brother). The index case is the first diagnosed case in an outbreak (in this case, the patient). In some instances, the primary case is also the index case, but often they are not the same. Secondary modes of transmission among humans can occur by different routes, such as contact with bodily fluids, exposure to airborne particles, fomites (objects that may be contaminated with viruses or bacteria), or via vectors. Seasonality and environmental change can greatly influence epidemics – think of birthing seasons and climate change.
Other drivers of zoonotic disease risk include intensive animal agricultural production, habitat destruction and resulting increase in human wildlife contact, as well as loss of biodiversity, leading to increased risk of pathogen emergence and spread.
That’s why it’s so important to learn more about the local landscape of human interactions with animals: for instance, what species do local humans interact with, and in what locations or settings? How specifically do they interact (i.e., what actions)? From taking in such information at a wide scale, clinicians can better understand modes of transmission and therefore create more targeted and effective interventions. They can also recognize risk in their patients due to contact with high risk animals and environments.
Some endemic zoonotic diseases (like brucellosis) regularly affect humans, but have limited transmission from person-person. Others may rarely jump to humans but when they do are capable of increased transmission and causing outbreaks (example: Nipah virus). Understanding the risk and mode of transmission for pathogens is essential for diagnosis and infection prevention and control.
Additionally, there is the potential for reverse zoonosis, also known as zooanthroponosis, whereby humans infect animals, which was seen during the COVID-19 pandemic. Clinicians need to be aware of the bidirectional (or multidirectional) potential for disease transmission.
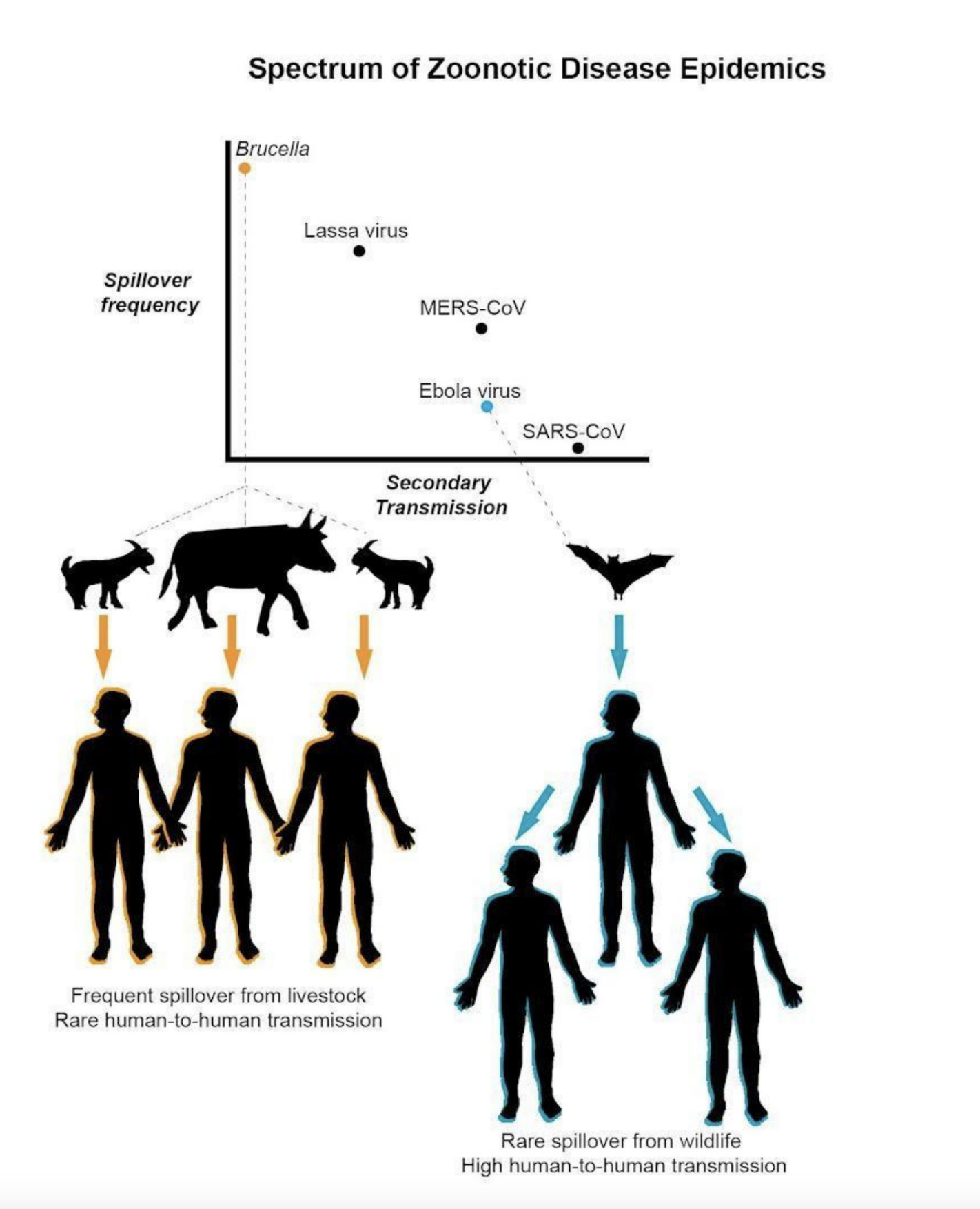
from Judson S, Rabinowitz P, (2021). Zoonoses and global epidemics. Current Opinion in Infectious Diseases. 9000.


Case Follow Up
additional community cases:
Subsequently, 17 other cases of Nipah virus infection are diagnosed in the community, including 2 relatives (aunt and father), 2 caregivers, and 5 inpatients at the same hospital.
It was suspected that the patient’s brother had contact with an infected bat pup or ate fruit contaminated by bat saliva. Around 20% of the bats collected from the outbreak area tested positive for Nipah virus (NiV) by RT-PCR, so the potential origin of the outbreak is spillover from bats. The subsequent cases were all from exposures to the primary case, either in the hospital or community.
*This case was based on a true case series of Nipah virus infections in Kerala, India.

Call to Action
Clinicians can take action to advance planetary health:
At the clinic:
Alert clinicians are key to detecting sentinel cases of zoonotic outbreaks, since you are the “first line” of eyes and ears who encounter a wide range of patients every day.
Include screening questions such as “do you or your family have contact with animals?” in your Social-E history.
If your suspect case could be infectious to others, implement infection control measures.
As a clinician who takes care of humans, you should be ready to communicate with veterinarians, who are trained to diagnose and treat infectious diseases in animals, including those that can be zoonotic. Furthermore, veterinarians may be more aware of infectious risks and can provide the insight needed to conduct a rapid and thoughtful response to emerging zoonoses.
Recommend patients maintain distance from wildlife and do not cohabitate with wildlife as pets or with other animals.
In your community:
Report any new cases of zoonotic diseases to health authorities; additionally report any state and nationally notifiable diseases.
Alert other health care providers to zoonotic risk in the community.
Raise awareness about local habitat destruction or increased animal contact.
Strengthen One Health efforts to bring local human care health providers and veterinarians together to better detect and respond to zoonotic and other common health threats.
At the societal level:
Pay attention to local legislation and use your vote to support effective policies and policy makers.
Advocate for increased attention to emerging zoonoses by meeting with lawmakers at all levels of governance (local, state, national) and writing op-eds on this issue.
Advocate (with veterinarians and environmental professionals and others) for improved management of human-wildlife contact, including habitat preservation and measures to preserve biodiversity in local environments.

Summary &
Key Learning Points
also available for download here:
Host risk factors for zoonotic infection:
“YOPI” : Young, Old, Pregnant, Immunocompromised
Contact with animals or animal products
Recent travel to high risk areas
Environmental risk factors:
Human contact with wildlife (or also domesticated animals)
Vector/rodent infestation
Local habitat destruction, loss of biodiversity
Flooding
Climate change, animal migration
History (“Social-E”):
Do you (or others nearby) have contact with animals at home or at work?
Recent travel and contact with animals or environments with wildlife?
Have you had any contact with sick animals? Has anyone around you been sick?
What kind of housing do you live in?
What kinds of things do you eat/drink? Do you eat/drink raw products?
Have you noticed any insects – or insect or animal bites?
Are you aware of any recent weather or environmental changes (flooding, etc.)?
Other risk data:
Health department reports, local veterinarians, farmers
Websites: CDC travel website, GIDEON, HealthMap
Physical:
Many zoonotic and vector borne diseases have non-specific presentations
Labs:
Access to rapid diagnostics, vaccines, and medical countermeasures remain limited. Therefore, high clinical suspicion and a detailed exposure history are important for clinical diagnosis and empiric treatment
Management:
Disease-specific treatment and support
Consider risk of person-to-person spread: infection control measures
Report cases to health authorities
Prevention:
Optimize host factors
Reduce exposure to animals, high-risk animal products, environments with animals
Raise awareness about local habitat destruction or increased animal contact.



Additional Resources
Datasets on infectious diseases (EIDs):
MicrobeNet (CDC’s online tool that helps clinicians identify pathogens)
Maps of the spread of infectious diseases:
ArboNET Disease Maps (CDC map of arboviruses in the US)
Map Gallery (WHO maps based on specific diseases)
HealthMap (worldwide map of infectious disease alerts)
Interactive maps | Infectious Diseases Data Observatory (many maps, mostly related to malaria and visceral leishmaniasis/VL)
Disease Maps | U.S. Climate Resilience Toolkit (US-wide maps of 7 vector-borne diseases)
ProMED (surveillance system reporting infectious disease outbreaks)
More information on clinicians’ role in preventing and detecting the next pandemic:
Reporting pathogen to CDC: How NNDSS Conducts Case Surveillance | CDC
More information on emerging zoonoses:

References
Clinical case data was obtained from: Pallivalappil B, Ali A, Thulaseedharan NK, et al. Dissecting an Outbreak: A Clinico-epidemiological Study of Nipah Virus Infection in Kerala, India, 2018. J Glob Infect Dis. 2020;12(1):21-27. Published 2020 Feb 19. doi:10.4103/jgid.jgid_4_19
Beevi, R L Sarita, Attayur P Sugunan, Govindakarnavar Arunkumar, D T Mourya, Manoj Murhekar, Clinical Manifestations of Nipah Virus–Infected Patients Who Presented to the Emergency Department During an Outbreak in Kerala State in India, May 2018, Clinical Infectious Diseases, Volume 71, Issue 1, 1 July 2020, Pages 152–157, https://doi.org/10.1093/cid/ciz789
Chandni R, Renjith TP, Fazal A, et al. Clinical Manifestations of Nipah Virus–Infected Patients Who Presented to the Emergency Department During an Outbreak in Kerala State in India, May 2018. Clinical Infectious Diseases. 2020;71(1):152-157. doi:10.1093/cid/ciz789
Emily S Gurley, Christina F Spiropoulou, Emmie de Wit, Twenty Years of Nipah Virus Research: Where Do We Go From Here?, The Journal of Infectious Diseases, Volume 221, Issue Supplement_4, 1 May 2020, Pages S359–S362, https://doi.org/10.1093/infdis/jiaa078
Giesecke J. Primary and index cases. Lancet. 2014 Dec 6;384(9959):2024. doi: 10.1016/S0140-6736(14)62331-X.
Islam M, Sazzad H, Satter S, et al. Nipah Virus Transmission from Bats to Humans Associated with Drinking Traditional Liquor Made from Date Palm Sap, Bangladesh, 2011–2014. Emerging Infectious Diseases. 2016;22(4):664-670. doi:10.3201/eid2204.151747.
Judson SD, Rabinowitz PM. Zoonoses and global epidemics. Curr Opin Infect Dis. 2021 Jul 26. doi: 10.1097/QCO.0000000000000749. Epub ahead of print. PMID: 34310453.
M. Jahangir Hossain, Emily S. Gurley, Joel M. Montgomery, Michael Bell, Darin S. Carroll, Vincent P. Hsu, P. Formenty, A. Croisier, E. Bertherat, M. A. Faiz, Abul Kalam Azad, Rafiqul Islam, M. Abdur Rahim Molla, Thomas G. Ksiazek, Paul A. Rota, James A. Comer, Pierre E. Rollin, Stephen P. Luby, Robert F. Breiman, Clinical Presentation of Nipah Virus Infection in Bangladesh, Clinical Infectious Diseases, Volume 46, Issue 7, 1 April 2008, Pages 977–984, https://doi.org/10.1086/529147
Luby SP, Gurley ES, Hossain MJ. Transmission of human infection with Nipah virus. Clin Infect Dis. 2009;49(11):1743-1748. doi:10.1086/647951
Lustgarten A. How Climate Change Is Contributing to Skyrocketing Rates of Infectious Disease. Propublica. Published May 7, 2020. https://www.propublica.org/article/climate-infectious-diseases.
Pallivalappil B, Ali A, Thulaseedharan NK, et al. Dissecting an Outbreak: A Clinico-epidemiological Study of Nipah Virus Infection in Kerala, India, 2018. J Glob Infect Dis. 2020;12(1):21-27. Published 2020 Feb 19. doi:10.4103/jgid.jgid_4_19
Thulaseedaran NK, Kumar KGS, Kumar J, Geetha P, Jayachandran NV, Kamalasanan CG, Mathew S, Pv S. A Case Series on the Recent Nipah Epidemic in Kerala. J Assoc Physicians India. 2018 Oct;66(10):63-67. PMID: 31317711.
Read More









